Updated 23rd February 2023
Whitepaper: An overview of our science




ZOE’s mission
ZOE is a health science company that was founded on the belief that novel digital technologies can enable human research at an unprecedented depth and scale, in order to tackle global health issues.
Our approach combines artificial intelligence, digital technologies and collaboration with leading scientists around the world. Our research ranges from the ongoing PREDICT studies, which is the world's largest in-depth nutritional research program, to an 800,000 person observational study to measure the accuracy of our AI diagnostic for COVID-19.
ZOE believes that recent technological advances make it possible to carry out high-quality human research in a real-world setting, and therefore answer questions that have not previously been feasible.
Combining large-scale biological data with machine learning and microbiome sequencing has enabled us to predict personal nutritional responses to foods and provide people with a better understanding of their unique metabolism and gut microbiome(1). These personalized insights can allow individuals to make impactful changes to improve their overall health.
An overview of the problem
Non-communicable diseases (NCDs) impacted by dietary risk factors, such as type two diabetes and cardiovascular disease, are the leading cause of mortality and morbidity in the developed world, and continue to increase at alarming rates(2,3,4,5). Unfortunately, current dietary and lifestyle approaches to tackle obesity and other major risk factors for these conditions are not achieving the positive impact that we all wish for. This is also true in developing countries, where a double burden of infectious and chronic diseases exists(6).
Reducing diet-related risk factors associated with these conditions is one of the most impactful ways to reduce ill-health, as well as lessening their detrimental impact on individuals and society as a whole(7,8,9).
However, our recent studies have demonstrated that our responses to food are unique, and therefore a “one-size-fits-all” approach to diet is unlikely to be the best strategy to enhance health(1). Therefore, ZOE’s ambition is to improve human health through precision nutrition by understanding how to eat the right way for our own biology and harness the potential power of the trillions of microbes in our gut.
ZOE’s scientific program
Our ongoing PREDICT program comprises the largest in-depth nutrition studies in the world to date. The PREDICT studies are designed so their data can be seamlessly combined in our machine learning models, enabling us to understand and predict personalized metabolic responses to foods, to provide people with nutritional recommendations tailored to their unique biology.
These clinical trials have allowed us to collect biological data in unprecedented detail from thousands of US and UK-based study participants, on hundreds of thousands of meals. Using this data, we have been able to characterize and unravel what determines the huge variability in human responses to food.
The first results from PREDICT have been published in the leading medical journal Nature Medicine in June 2020. These results have been used to create personalized “ZOE Scores” for individuals who use the ZOE product. More details about the PREDICT program can be found here.
Rethinking the future of nutrition
For many years, medication has been used as the first line of therapy for treating NCDs, yet dietary approaches have the potential to be more effective(7,8,9). Nutritional science is now advancing at a rapid pace. However, due to the complexity of our bodies (with our thousands of biochemical pathways) and of foods (over 26,000 chemicals have been identified in our food(10), we are only starting to scratch the surface in understanding how food impacts our health at an individual level.
In addition, recent research has highlighted the multiple interacting pathways linking diet, microbiome and health(11,12,13,14). This has revealed how our microbiome can modulate the impact of food to transform our long term health and weight.
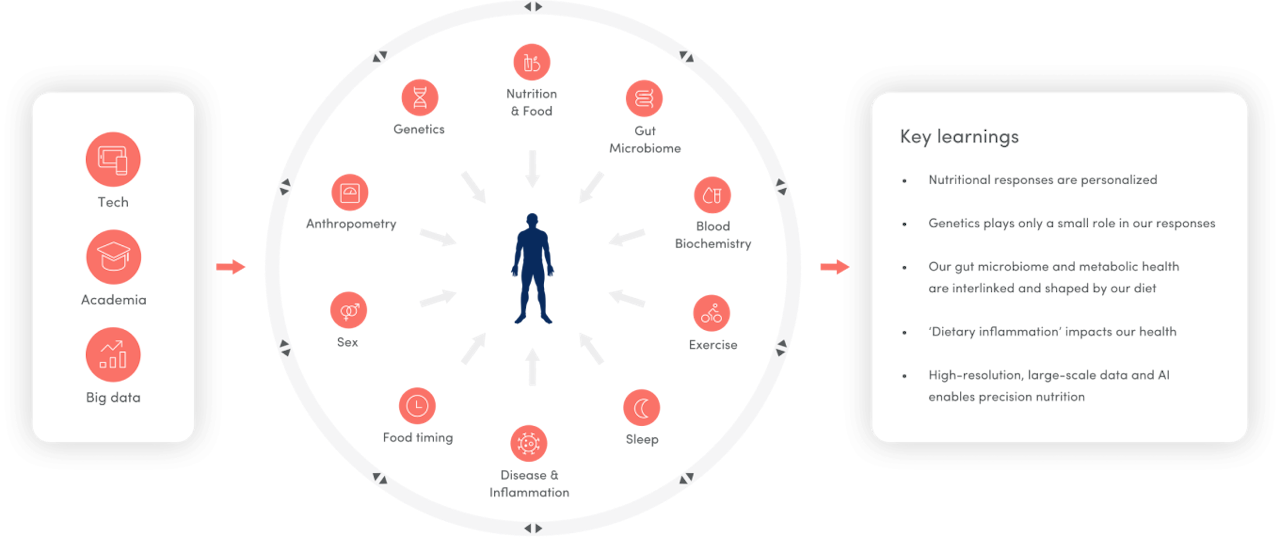
A key focus of ZOE’s PREDICT research program has been to explore and untangle the many interrelated and multidirectional determinants of our responses to food. This has allowed us, for the first time, to combine highly detailed analysis of thousands of gut metagenomes (all of the genes found in our gut microbes combined), with a detailed understanding of the individual’s characteristics (e.g. genetics, circulating blood metabolites), their metabolic responses to foods and health measures(1).
A complex chain of unhealthy metabolic effects can be triggered after we eat. (Figure 2). Eating typical meals (which include protein, carbohydrates and fat) elicits short-term changes in blood fat and glucose levels (postprandial lipemia/ glycemia), as well as other circulating metabolites.
Excessive lipemia and glycemia can overwhelm the body's normal, healthy regulatory responses, triggering a wide variety of unfavorable responses in blood lipids, rebound hypo-glycaemia, immune measures and hunger. Repeated often enough, these can lead to long-term inflammation, weight gain and chronic diseases such as diabetes and heart disease(15,16,17,18).


Weight gain has typically been attributed to a failure to maintain energy balance (i.e., calories in = calories out)(10). But we now know that energy expenditure is highly dynamic and individual, and that both our microbiome and the food we eat can impact our metabolism. This explains, in part, why calorie reduction diets tend to fail for most individuals and is where personalized food guidance focused on quality for each individual rather than calories could have a big impact(20).
Key learnings from our research
The key messages from ZOE’s research so far can be summarized in six areas:
1. Individual responses to the same foods vary
We have found dramatic inter-individual variability between how healthy individuals respond to the same foods(1) (as illustrated in Figure 3). For example, after a standardized high fat/high carbohydrate meal the variability between individuals in postprandial lipaemic and glycaemic responses was 103% and 68% respectively (coefficient of variation (CV)), amongst 1,102 healthy individuals in the PREDICT 1 study. This was substantially higher than fasting TG and glucose variability (50% and 10% CV respectively), showing that measuring an individuals postprandial response allows better discrimination between indivudals in their metabolic health. Importantly these findings confirm that there is no ‘one-size-fits-all’ approach to nutrition, and point to the need for personalized guidance in eating that takes into account an individual’s unique biology.


2. Our gut microbiome plays an important role in our metabolic health
We have found strong links between the microbes in our gut and our individual metabolic responses to food(21,22). We have also revealed links between specific foods and dietary patterns, and individuals’ microbes in their gut at an unprecedented resolution(21). Further, our research shows that diet rich in minimally processed, high-fibre, plant-based foods is linked with “good” gut microbes linked to healthy metabolic responses. On the other hand, a diet high in highly processed foods is associated with “bad” microbes. An exciting and novel finding is that genetics only plays a minor role in shaping our microbiome — even identical twins share only 34% of the same gut microbes (compared with 30% in unrelated individuals) (unpublished data). Thus the gut microbiome is an important and modifiable target for personalized nutrition.
3. ‘The metabolic cascade’ can have a large impact on our health
This is the complex chain of effects that can be caused by what we eat(23). Our research shows that the huge variability in lipemic and glycemic responses is also associated with large variability between individuals in other measures, including insulin, immune cell parameters and atherogenic lipoproteins. Our “good” gut microbes are associated with a favourable metabolic response to foods, as well as lower levels of belly fat(22).
4. We are not prisoners of our genes
By looking at the many interrelated determinants of responses to food (Figures 4a-c), we have found, for the first time, that genes only play a minor role in determining our responses to food (30% for glucose, 4% for triglycerides and 9% for insulin; calculated genetic variances), and that even identical twins respond very differently to the same foods(1). This shows that our health is not solely predetermined by our genes and that we do have the power to improve it through diet and lifestyle strategies tailored to our biology.

.")
5. Weight gain may not be just a result of too many calories
Our research confirms that we should look beyond calories when striving to maintain body weight. We found that different foods with the same number of calories is linked to different levels of hunger, insulin sensitivity and calorie consumption at the next meal which is sustained over the following 24-hour period(24).
6. Machine learning can be used to generate personalized nutrition advice
By measuring thousands of people’s metabolic responses to standardized test meals, as well as those consumed in free-living conditions, we have been able to use machine learning models to generate meaningful, personalized “ZOE Scores” for any food or meal. These scores provide insights into the kinds of foods that improve overall health, the gut microbiome and reaching a healthy weight, improve an individual’s gut microbiome, and help them reach a healthy weight, which may improve long-term health outcomes. As our studies continue, we expect these scores to further improve.
Our research has shown that there is huge inter-individual variability in our responses to food which is mainly determined by non-genetic factors including the gut microbiome. Our ongoing ambition at ZOE is to take the latest discoveries from our research and make these available to everyone. We will do this by providing tests and personalized ZOE Scores that reflect our latest research findings, using AI models to make precision nutrition a reality.
Authors




Continue reading
Sources
Berry SE, Valdes AM, Drew DA et al. Human postprandial responses to food and potential for precision nutrition. Nat Med. 2020;26:264-73. Available from: doi:10.1038/s41591-020-0934-0
Menke A, Casagrande S, Geiss L, Cowie CC. Prevalence of and Trends in Diabetes Among Adults in the United States, 1988-2012. JAMA. 2015 Sep 8;314(10):1021-9. doi:10.1001/jama.2015.10029
Hales CM, Carroll MD, Fryar CD, Ogden CL. Prevalence of obesity and severe obesity among adults: United States, 2017-2018. NCHS Data Brief, no 360. Hyattsville, MD: National Center for Health Statistics, 2020. Available from: https://www.cdc.gov/nchs/data/databriefs/db360-h.pdf
GBD 2015 Risk Factors Collaborators. Global, regional, and national comparative risk assessment of 79 behavioural, environmental and occupational, and metabolic risks or clusters of risks, 1990–2015: a systematic analysis for the Global Burden of Disease Study 2015. Lancet. 2016;388(10053):1659-1724. doi:10.1016/S0140-6736(16)31679-8
GBD 2017 Diet Collaborators. Health effects of dietary risks in 195 countries, 1990–2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet. 2019;393:1958-72. doi:10.1016/S0140-6736(19)30041-8
Bygbjerg IC. Double Burden of Noncommunicable and Infectious Diseases in Developing Countries. Science. 2012 Sep;337:1499-501. doi:10.1126/science.1223466
Galani C, Schneider H. Prevention and treatment of obesity with lifestyle interventions: review and meta-analysis. Int J Public Health. 2007;52:348-59. doi:10.1007/s00038-007-7015-8
Slawson DL, Fitzgerald N, Morgan KT. Position of the Academy of Nutrition and Dietetics: The Role of Nutrition in Health Promotion and Chronic Disease Prevention. J Acad Nutr Diet. 2013 Jul;113(7):972-9. doi:10.1016/j.jand.2013.05.005
Schulze MB, Martínez-González MA, Fung TT et al. Food based dietary patterns and chronic disease prevention. BMJ. 2018;361:k2396. doi:10.1136/bmj.k2396
Barabási A, Menichetti G & Loscalzo J. The unmapped chemical complexity of our diet. Nat Food. 2020;1:33–37. doi:10.1038/s43016-019-0005-1
Zmora N, Suez J & Elinav E. You are what you eat: diet, health and the gut microbiota. Nat Rev Gastroenterol Hepatol. 2019;16:35-56. doi:10.1038/s41575-018-0061-2
Menni C, Jackson MA, Pallister T et al. Gut Microbiome Diversity and High-Fibre Intake Are Related to Lower Long-Term Weight Gain. Int J Obes. 2017 Jul;41(7):1099-105. doi:10.1038/ijo.2017.66
Singh RK, Chang H-W, Yan D et al. Influence of diet on the gut microbiome and implications for human health. J Transl Med. 2017;15:73. doi:10.1186%2Fs12967-017-1175-y
Telle-Hansen VH, Holven KB & Ulven SM. Impact of a Healthy Dietary Pattern on Gut Microbiota and Systemic Inflammation in Humans. Nutrients. 2018 Nov;10(11):1783. doi:10.3390%2Fnu10111783
Kolovou GD, Mikhailidis DP, Kovar J et al. Assessment and clinical relevance of non-fasting and postprandial triglycerides: an expert panel statement. Curr Vasc Pharmacol. 2011;9(3):258–270. doi:10.2174/157016111795495549
Astley CM, Todd JN, Salem RM et al. Genetic evidence that carbohydrate-stimulated insulin secretion leads to obesity. Clin Chem. 2018;64(1):192–200. doi:10.1373%2Fclinchem.2017.280727
Blaak EE, Antoine J-M, Benton D et al. Impact of postprandial glycaemia on health and prevention of disease. Obes Rev. 2012;13(10):923-84. doi:10.1111%2Fj.1467-789X.2012.01011.x
DECODE Study Group, European Diabetes Epidemiology Group. Glucose tolerance and cardiovascular mortality: comparison of fasting and 2-hour diagnostic criteria. Arch Intern Med. 2001;161:397-405. doi:10.1001/archinte.161.3.397
Hill JO, Wyatt HR & Peters JC. Energy Balance and Obesity. Circulation. 2012;126:126-32. doi:10.1161/CIRCULATIONAHA.111.087213
Spector T & Gardner C. Challenges and opportunities for better nutrition science—an essay by Tim Spector and Christopher Gardner. BMJ. 2020;369:m2470. doi:10.1136/bmj.m2470
Spector T, Asnicar F, Berry S et al. Microbiome Signatures of Nutrients, Foods and Dietary Patterns: Potential for Personalized Nutrition from The PREDICT 1 Study. Curr Dev Nutr. 2020 May;4(2):1587. doi:10.1093/cdn/nzaa062_044
Berry S, Ordovas J, Asnicar F et al. Influence of Gut Microbial Communities on Fasting and Postprandial Lipids and Circulating Metabolites: The PREDICT 1 Study. Curr Dev Nutr. 2020 May;4(2):1547. doi:10.1093/cdn/nzaa062_004
Berry S, Mazidi M, Franks P et al. Impact of Postprandial Lipemia and Glycemia on Inflammatory Factors in over 1,000 individuals in the US and UK: Insights from the PREDICT 1 and InterCardio studies. Curr Dev Nutr. 2020 Jun;4(2):1518. doi:10.1093/cdn/nzaa068_003
Berry S, Wyatt P, Franks P et al. Effect of Postprandial Glucose Dips on Hunger and Energy Intake in 1102 Subjects in US and UK: The PREDICT 1 Study. Curr Dev Nutr. 2020 Jun;4(2):1161. doi:10.1093/cdn/nzaa063_009

